Giardia duodenalis
Synonymous: G. intestinalis, G. lamblia
Contributor: Andre Buret
Biology: Protozoan parasite in the family Hexamitidae. Giardia duodenalis was discovered in 1681 by Anton van Loeuwenhoek, the inventor of the light microscope, from his own stools. G. duodenalis can infect a wide variety of mammals and humans, as well as birds. The taxonomy and speciation of G. duodenalis is subject to debate. To date, G. duodenalis has been reported to exist in 8 distinct genetic “assemblages” or “genotypes”. Assemblages A and B can infect human hosts.
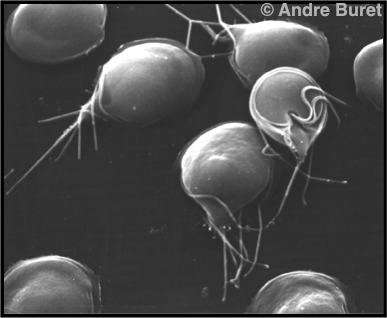
Figure 1. Scanning electron micrograph of the motile trophozoite form of the Giardia parasite. The ventral adhesive disk is used by the trophozoites to attach to the intestinal surface.
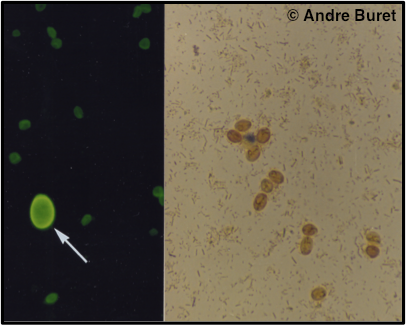
Figure 2. The 10 µm faecal cysts isolated from faecal samples can be visualized under light microscopy using fluorescent dyes (left, arrow, beside the smaller oocysts of Cryptosporidium), or when stained with iodine (right).
Life Cycle: The flagellated trophozoite stage (Figure 1) excysts in the duodenum, upon exposure to bile. Trophozoites live freely within the upper small intestine, and cause the pathogenic effects of the organism without invading host tissues. Trophozoites, which multiply by binary fission, encyst in the large intestine, and cysts are released in the faeces. The environmentally resistant cysts (Figure 2) ensure parasite transmission.
Figure 3. G. duodenalis life cycle (Source: CDC).
Transmission: Infection occurs following ingestion of infectious cysts either directly via the fecal-oral route, or indirectly via contaminated food or water. Waterborne outbreaks of giardiasis are common. G. duodenalis is the most common cause of waterborne disease in developed countries of the World. At least some of the genetic “assemblages” of Giardia may be transmitted from animals to humans and vice-versa.
Prevalence: G. duodenalis exists worldwide, and is very common. Prevalence of 100% in children populations have been reported (1).
Susceptible Populations: Immunocompromised people, travellers, young children.
Symptoms: The clinical manifestations of G. duodenalis infection are highly variable. Infected hosts may present with a spectrum of symptoms ranging from asymptomatic carriage to acute or chronic symptomatic infection that manifests as diarrheal disease (1). In the majority of cases, the gastrointestinal symptoms associated with giardiasis include diarrhea, bloating, abdominal pain, nausea, vomiting, as well as anorexia and failure to thrive. Most commonly, symptoms start 7 to 10 days after infection (range 3-25 days post-infection). Some hosts may develop more complex chronic symptoms, including post-infectious Irritable Bowel Syndrome (2).
Treatment: Although not fully effective, Metronidazole (flagyl) remains the most commonly used treatment for giardiasis.
Control Measures: Use of decontaminated, filtered water. G. duodenalis is resistant to chloride. Good hygiene is important, washing of fruits and vegetables is recommended where faecal contamination is a risk.